Clinical researchers at the University of Tartu in Estonia published findings connecting a rare variant in the MGRN1 gene to congenital heart malformations. The April 4, 2026 research note linked MGRN1 to a clearer prenatal risk question. This specific discovery marks the first time science has linked the gene to human embryonic development or any clinical disease. Results from the study clarify why certain structural defects occur during the earliest stages of fetal growth. Geneticists previously categorized the MGRN1 gene as a biological unknown in human cardiac health. Identifying this correlation allows medical professionals to provide more accurate diagnostics for expectant parents facing complicated pregnancies.
Congenital heart disease affects approximately 1% of all live births globally, according to data from the World Health Organization. While environmental factors and known chromosomal abnormalities explain many cases, a meaningful portion of heart defects lacks a clear genetic origin. Researchers within the Human Genetics Research Group focused on these unexplained occurrences to find hidden drivers of malformation. Success in mapping the MGRN1 variant suggests that more undiscovered genes may reside in the darker corners of the human genome. Finding these hidden triggers is essential for reducing the global burden of infant mortality related to cardiac issues.
MGRN1 Gene Discovery and Human Development
Mapping the human genome revealed thousands of genes, yet the specific function of many remains elusive. MGRN1, or Mahogunin Ring Finger 1, was previously studied in rodent models where it appeared to influence neurological health. Estonian scientists, however, found that its role in humans is far more critical during the first trimester of pregnancy. Proteins produced by this gene act as cellular managers, directing the flow of structural development in the heart. When the gene carries a defect, the heart fails to form the complex valves and chambers necessary for post-natal survival.
The discovery will help doctors better recognize similar cases in the future and improve the counseling and treatment offered to affected families, according to the Human Genetics Research Group of the University of Tartu Faculty of Medicine.
Precision in genetic mapping provides a new lens for viewing fetal pathology. Before the announcement on April 4, 2026, clinicians often had to tell families that the cause of a heart defect was simply unknown. Such uncertainty adds serious emotional weight to an already difficult medical situation. Knowing the exact gene involved allows for targeted screening and a clearer understanding of the risk for future pregnancies. Families can now make decisions based on molecular evidence rather than statistical guesswork.
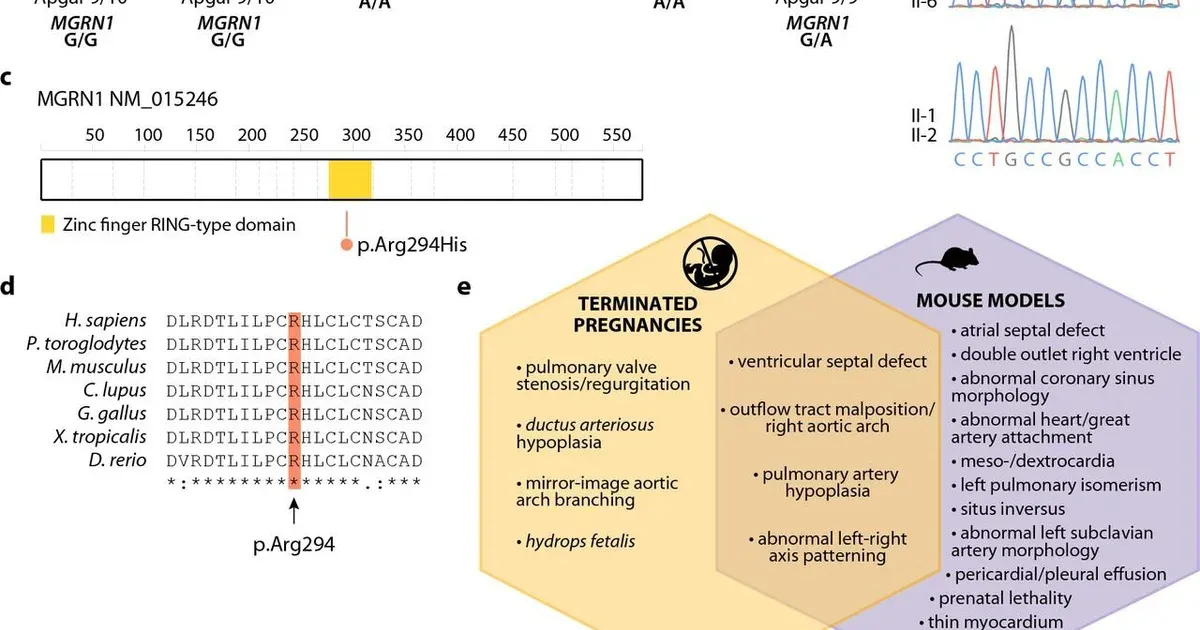
Biological systems rely on E3 ubiquitin ligases like MGRN1 to maintain cellular order. These ligases identify and tag proteins that need to be removed or moved to different parts of the cell. During cardiac morphogenesis, the timing of protein degradation must be perfect. If a signaling protein remains active for too long because MGRN1 is broken, the heart tissue may grow in the wrong direction. Such errors lead to conditions like septal defects or transposition of the great arteries. These malformations frequently require invasive surgery shortly after birth.
Cellular traffic jams are often the root cause of developmental failure. If the MGRN1 protein cannot clear out debris, the cells responsible for building the heart walls lose their way. Researchers at the University of Tartu used advanced sequencing techniques to observe these tiny molecular failures. Their work suggests that MGRN1 interacts with specific signaling pathways that define the left and right sides of the body. Disrupting this symmetry is a hallmark of the most severe congenital heart conditions seen in neonatal wards. Supporting data from the study indicate that even a single nucleotide change can halt the entire process.
Improving Prenatal Diagnostics and Family Counseling
Prenatal screening technologies have advanced rapidly, but their utility is limited by the library of known genetic markers. Including MGRN1 in standard screening panels will provide a more thorough view of fetal health. High-risk families, especially those with a history of cardiac issues, stand to benefit the most from this updated genetic catalog. Early detection often allows for specialized delivery plans at hospitals equipped with pediatric cardiology units. This foresight can be the difference between a successful intervention and a tragic outcome.
Genetic counseling becomes a precise tool when clinicians possess specific data points. Knowing that a mutation is inherited or de novo helps parents understand the likelihood of the condition recurring. This discovery also opens doors for future therapeutic research into how E3 ubiquitin ligases might be stabilized during pregnancy. While gene editing remains a distant prospect for cardiac defects, diagnostic clarity is an immediate benefit of the Tartu findings. Doctors can now offer a plan for care that starts in the womb. Every new gene identified brings the medical community closer to a total understanding of human development.
MGRN1 Finding Sharpens Prenatal Risk Research
The MGRN1 finding gives researchers a clearer target for studying fetal heart formation. It does not create an immediate treatment, but it may help doctors identify risk earlier and design better follow-up studies.